“Prior to the start of the SYNTAX trial (sponsored in 2005 by Boston Scientific), the trial designers’ concern was the accurate, semi-quantitative assessment—by surgeons and interventional cardiologists—of the extent and anatomical complexity of the coronary artery disease (CAD) before inclusion of patients in the landmark SYNTAX trial. Originally, the anatomical SYNTAX Score was simply a scoring tool to force the physicians to meticulously inspect and assess the anatomical complexity of the coronary anatomy visualized either by invasive cine angiography (ICA) or more recently by non-invasive computerized tomographic angiography (CTA).
To create the anatomic SYNTAX tool, numerous existing scores stemming from the literature were combined: the Leaman score, ACC/AHA lesions classification system, a chronic total occlusion score, the Medina score, a thrombus score, a calcification score and so on. This amalgam of scores were then organized in a complex hierarchical algorithm.1
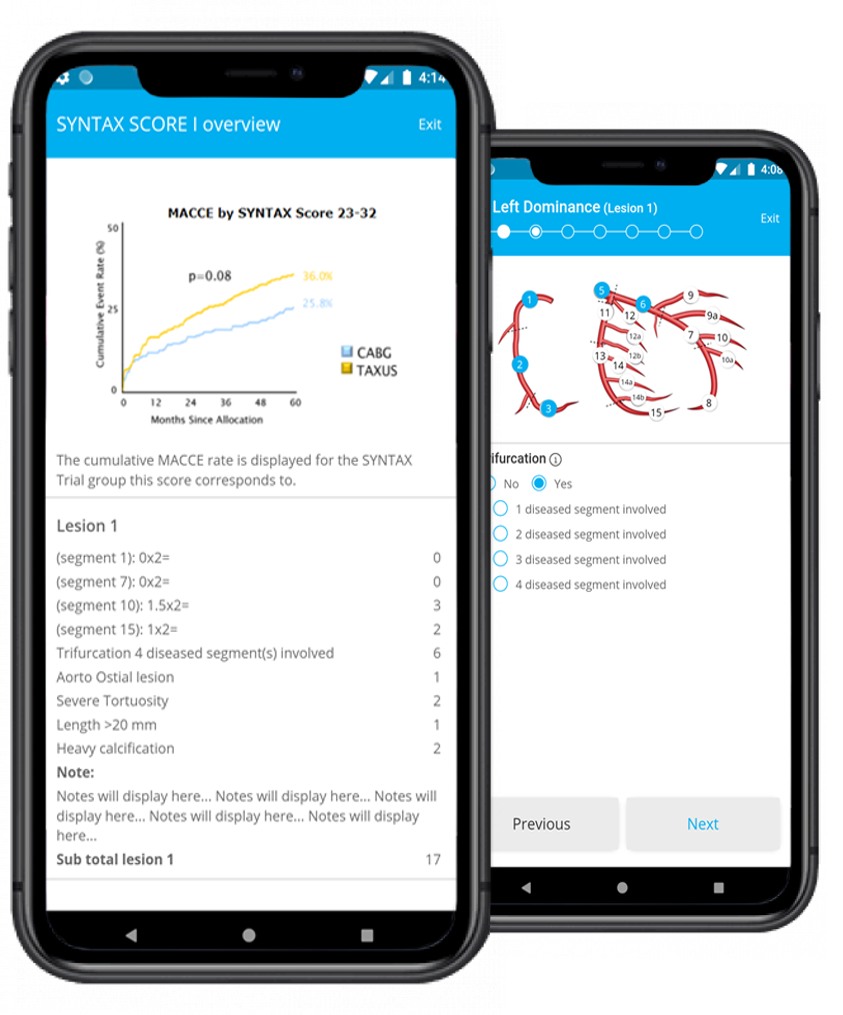
The prognostic value of the score in predicting the rates of major adverse cardiac and cerebrovascular events (death, stroke, myocardial infarction, or revascularization) in the various SYNTAX scores substrata (<22, <33) of patients treated by either percutaneous coronary intervention (PCI) or coronary artery bypass grafting (CABG) became only evident once the outcome of the SYNTAX trial was unraveled in 2009 (1 year follow up) and 2013 (5 years follow up). 2, 3 Of note, the prognosis of surgical cases was hardly affected by the anatomical SYNTAX score since the surgeon had the option to “bypass” all these anatomical complex obstacles.
At the same time, it was realized that the prognosis of a surgical case was more related to comorbidities and clinical characteristic best described, for instance, by the EuroSCORE, STS score, and ACEF score.
The undermentioned table summarizes the evolution of the anatomic SYNTAX Score 2-4, following its merging with clinical characteristics and comorbidities (SYNTAX Score II [Lancet, 2013], SYNTAX Score 2020 [lancet 2020] 5, 6 and logistic SYNTAX Score) 7-11 and its further refinement after functional and weighing adjustment (so called functional score) using physiological assessment such as instantaneous wave-free ratio (iFR), fractional flow reserve (FFR) or quantitative flow ratio (QFR) 12 (SYNTAX Score III = anatomy + comorbidity + functionality). 13-17”
It is important to note that the safety and effectiveness of drug-eluting stents have not yet been fully established in complex and extensive CAD. Physicians are strongly encouraged to review the indications, contraindications, warnings and instructions included in the products’ Directions for Use of the various stents available on the market.
The parent SYNTAX Score and its derived variants intended to provide therapeutic advice or guidance as to appropriate treatment strategies for individual patients. However, risks and benefits should be carefully considered for each patient taking into account all available data and treatment options.Physicians and other healthcare providers should always exercise their own clinical judgement for any given situation follow individual product instructions.
The SYNTAX Score and related variants were developed under the leadership of the SYNTAX and Multivessel TALENT Steering Committee, in collaboration with the CORRIB Core Lab of the National University of Ireland in Galway: smartphone application and adapted Website were produced by Sahajanand Medical Technologies (SMT) and the CORRIB Core Lab to support practitioners in their treatment decision making for patients with complex CAD.