introducing
Syntax Score 2020
The SYNTAX Score 2020 guides the individual treatment decision making between PCI and CABG for patients having three-vessel disease with/without left main on the basis of 5 years MACCE and 10 years all-cause mortality.




Anatomy (ICA), population strata outcome, Population: PCI and CABG.Predicts MACCE prognosis from 1 to 5 years in the SYNTAX trial (PCI vs. CABG in three-vessel disease and left main)1-3 and mortality up to 10 years in the SYNTAXES study.
Anatomy (ICA) and comorbidity, Population: individualized outcome for “all-comers” PCI Predicts all-cause mortality at 2 years in “all-comers” PCI.
Anatomy (CTA), comorbidity, and functionality (FFRCT), Population: PCI and CABG Treatment decision making between PCI and CABG in 3VD & LM based solely on multi-slice CT scan with FFRCT in the SYNTAX III REVOLUTION trial.
Anatomy (ICA and CTA) and functionality (iFR, FFR, FFRCT, QFR), Population: PCI and CABG Treatment decision making based on anatomy and functionality.
Anatomy (ICA) and comorbidity, Population: PCI versus CABG. Predicts 4-year all-cause mortality in the SYNTAX trial.
* The SYNTAX Score II will be superseded by SYNTAX Score 2020.
Anatomy (CTA), comorbidity, and functionality (FFRCT), Population: CABG Planning and execution of surgery in 3VD & LM applying SYNTAX Score III erived solely on CTA scan with FFRCT (the FASTTRACK CABG trial, First in men).
Anatomy (ICA) and comorbidity, Population: PCI versus CABG Predict 5-year MACE and 10-year all-cause mortality based on cross validation in the SYNTAX trial and on external validation in the FREEDOM, BEST, and PRECOMBAT trials
**CABG: coronary artery bypass grafting; CTA: computed tomography angiography; FFR: fractional flow reserve; FFRCT: fractional flow reserve derived from CTA; ICA: invasive coronary angiography; iFR: instantaneous wave-free ratio; QFR: quantitative Flow Ratio; PCI: percutaneous coronary intervention; 3VD: three-vessel disease; LM: left main:.
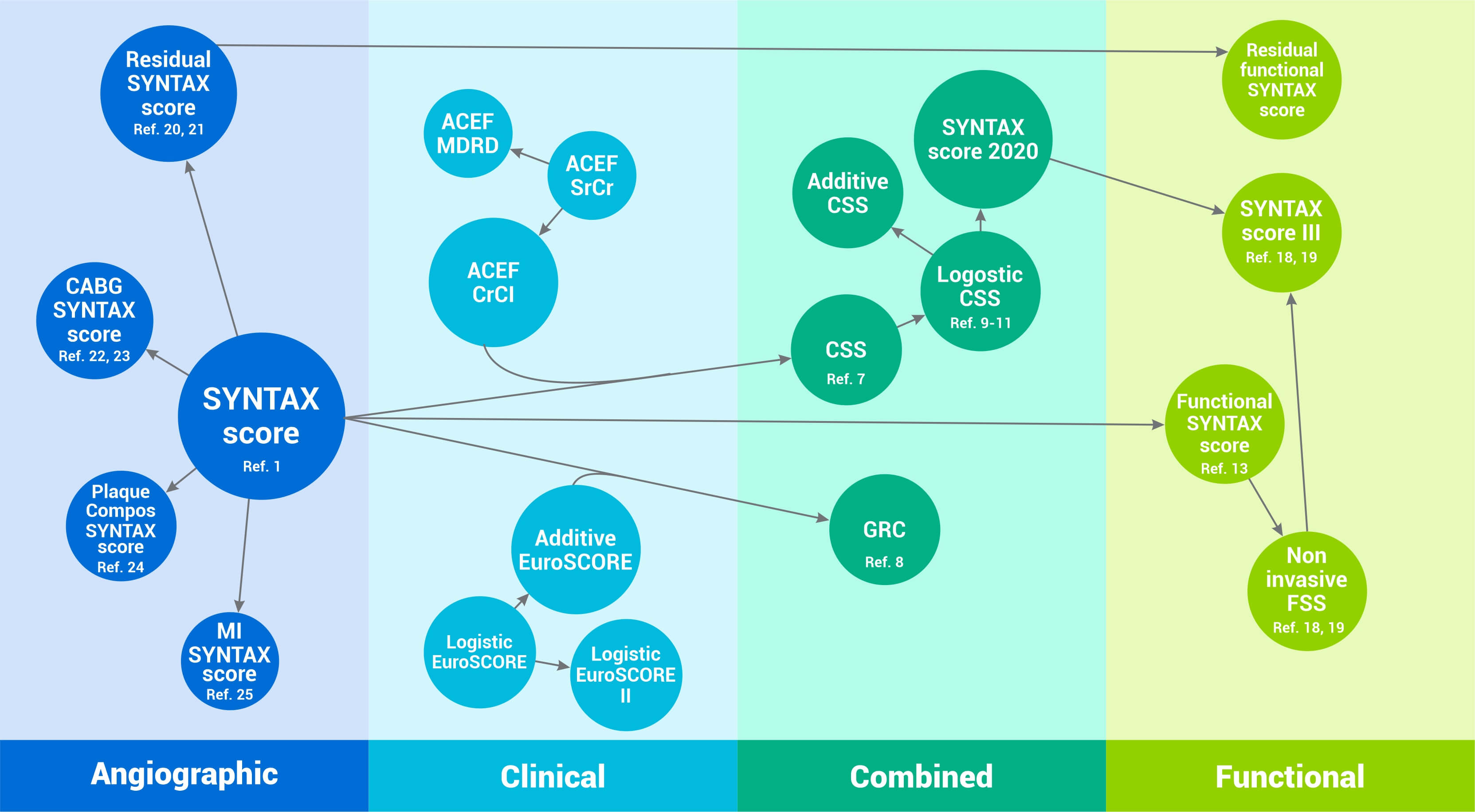
“Prior to the start of the SYNTAX trial the trial designers’ concern was the accurate, semi-quantitative assessment—by surgeons and interventional cardiologists—of the extent and anatomical complexity of the coronary artery disease (CAD) before inclusion of patients in the landmark SYNTAX trial. Originally, the anatomical SYNTAX Score was simply a scoring tool to force the physicians to meticulously inspect and assess the anatomical complexity of the coronary anatomy visualized either by invasive cine angiography (ICA) or more recently by non-invasive computerized tomographic angiography (CTA).
To create the anatomic SYNTAX tool, numerous existing scores stemming from the literature were combined: the Leaman score, ACC/AHA lesions classification system, a chronic total occlusion score, the Medina score, a thrombus score, a calcification score and so on. This amalgam of scores were then organized in a complex hierarchical algorithm.1
Read More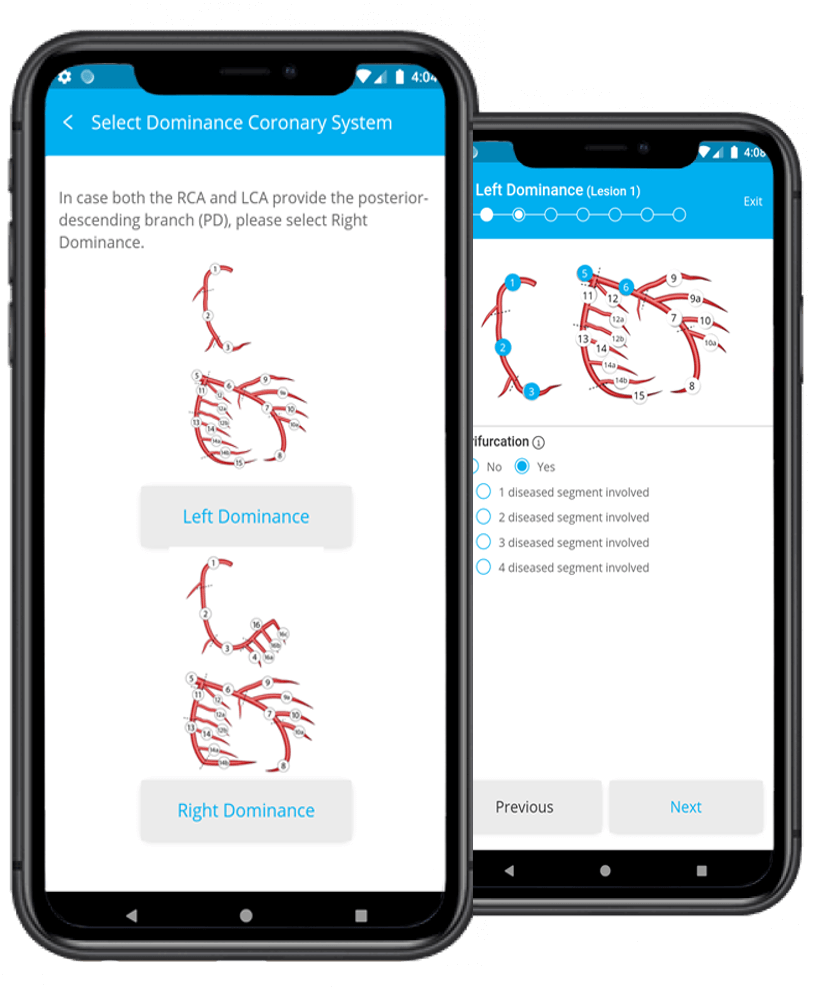


Established professor of interventional medicine and innovation
Professor Patrick Serruys is a world-renowned expert in interventional cardiology and imaging with more than four decades of experience in clinical trials and innovation in medicine. He has pioneered several interventional procedures and devices such as BMS, DES, BRS and TAVI as well as imaging techniques.These techniques have been used to assess many pharmacological trials aiming at resolving the issue of restenosis.

Director of Coronary Imaging and Atherosclerosis Research
Dr. Yoshinobu Onuma, MD, PhD is a leading expert in the field of noninvasive and invasive coronary imaging and novel coronary devices such as bioresorbable scaffolds. His expertise includes quantitative coronary angiography (2-dimensional, 3-dimensional and bifurcation-dedicated), Syntax Score and multi-slice computed tomography. He holds the position of professor of interventional cardiology at the National university of Ireland Galway.

Clinical Trial Coordinator
MA Morel is an experienced clinical trial project manager in Interventional Cardiology and has coordinated many device studies including landmark trials such as BENESTENT and SYNTAX. She has been key in developing the web-based SYNTAX Score clinical tool which has had great impact into the current cardiology clinical practice. Currently she is senior Clinical Trial Coordinator at NUI Galway